



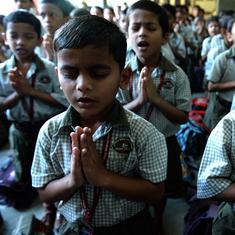






The signboards clearly indicated where the Covid-19 vaccination centre was situated at Delhi’s Lok Nayak Jai Prakash Narayan Hospital. Yet, the centre, spruced up with welcome signs and a photo booth, was sparsely populated on Tuesday morning. The registration queue manned by two policemen had barely ten people in line for the vaccine. Most of them were hospital staffers wearing their scrubs.
Outside the Delhi government-run hospital, 50-year-old daily-wage earner Prem Nath and his wife Asha Devi, 48, stood waiting for the bus to get back to their home in Dwarka, West Delhi. They did not know the hospital had a centre where they could avail the coronavirus vaccines free of cost.
“We know there is a vaccination going on [in the country] but we do not know how to get it,” said Nath, a diabetic patient, who had accompanied Devi, a domestic worker, to the hospital to get her treated for the aches she felt in her jaw.
“From where will we get it?” he asked this reporter.
On March 1, the Centre extended its vaccination drive from frontline health workers to senior citizens above the age of 60 years and those above 45 with comorbidities. In this phase of the drive, twice as many private hospitals as serving as vaccination centres than government hospitals. While government hospitals are offering the vaccines for free, private hospitals have been allowed to charge a maximum of Rs 250 per dose.
Ten days into this second phase of vaccinations, doctors and health workers in Delhi have noticed a trend. “It is mostly educated people who are coming while the rest are hospital staff,” said a doctor from the radiology department manning the vaccination centre at Lok Nayak Jai Prakash Narayan Hospital. “People from the poorer sections are not coming. They are not aware of this.”
At the Central government-run Ram Manohar Lohia Hospital in the capital, doctors at the empty waiting area for the vaccine said that “90 per cent of the beneficiaries belonged to the middle class and upper middle class”.
“A lot of those who are on high posts, who live around the area, and are comfortable with technology are coming,” said a doctor at the registration desk at the hospital who did not want to be identified. “They are very much aware of the vaccine and possible side effects,” he said.
The class divide isn’t just noticeable in Delhi. In Mumbai, doctors heading municipal-run hospitals told The Times of India that only “elite people” – many of whom were visiting the hospitals for the first time – were showing up to take the vaccines.
The newspaper reported a similar situation in Bengaluru where doctors said that elders from poorer sections were yet to avail the vaccines. “We are yet to see our regular patients from slums coming to receive the vaccine,” said an unidentified city-based doctor.
Meanwhile, social media is flooded with pictures of affluent Indians posing at photo booths after receiving the vaccine.
Falling through the gaps
The class divide in Covid-19 vaccinations could be attributed to a number of reasons, said experts.
“The information has only been shared with a certain class,” said Dr Sylvia Karpagam, a public health doctor and researcher who lives in Bengaluru. The other reason was the use of technology: vaccine beneficiaries need to register on CoWin, a digital platform built by the government.“Online registration is a big barrier,” said Karpagam.
For those who are unable to register online, hospitals are meant to provide walk-in facilities. But the central government has asked states to “encourage” online registrations. A press release issued by the Press Information Bureau on March 9 explained the rationale behind this move: “...to facilitate the entire process by making it more convenient for the citizen, as well as giving authorities a forward view of expected demand to plan accordingly and avoid over-crowding.”
But instead of making it convenient, online registration is leading to the exclusion of the poor who lack smartphones and access to the internet, say health experts.
Said Dr KR Anthony, a Kochi-based public health consultant, “Technology coming in the way of registration is a handicap so naturally there is an exclusion and skewing of a large chunk to sophisticated and literate people.”

Building awareness
To ensure everyone has access to the vaccine, the government needs to create a better framework, said experts. Before devising a strategy, it was important to first understand who the drive aims to target. “Whom do you want to give it to and how are you going to give it?” asked Sulakshana Nandi of Jan Swasthya Abhiyan.
If the government aims to vaccinate the elderly population, then it would have to make it available for them closer to their homes, Nandi said. “We are seeing the elderly standing in long lines,” she said. “Clearly, there has been no effort to design a full vaccination strategy.”
Another approach could be measuring the entitlement to the vaccine by mapping out vulnerabilities and accordingly targeting specific groups. “The more the risk borne, the more the entitlement,” said T Sundararaman former director of the National Health Systems Resource Centre, an advisory body of the Union Ministry of Health and Family Welfare.
Apart from age and comorbidities, occupation could also be taken into account. “If you are a migrant worker, or working in a factory, these are also vulnerabilities,” Sundararaman said. “When we were talking about virus control, we were talking about occupation. But when we are talking about vaccine need, we have completely forgotten about this factor.”
This, however, may not be as simple in urban areas where the poor often lack access to primary healthcare in the public sector.
“Our entire urban health system is very confused throughout the country,” said Prabir Chatterjee, a doctor currently based in rural Bengal, who has spent several years working in the government’s pulse polio and other routine immunisation programs. “If you want to do it [vaccination] in slum areas, you have to have centres there which are run by the government.” Currently, such infrastructure is missing in many urban settlements.
Chatterjee said the government would have to proactively pursue working-class beneficiaries to ensure a more equitable access to the Covid-19 vaccines. Sundararaman agreed: “We have to overcome this [asymmetry] because there are different degrees of awareness.” He recommended that a certain amount of vaccines be reserved for vulnerable sections through public health systems.
Other health researchers emphasised that the government would need to start by improving its outreach for Covid-19 vaccination. “They could have seen this as an opportunity and recruited health workers, nurses, auxiliary nurses and midwives, and could have used them to strengthen the outreach,” Nandi said.
Another necessary step would be building trust within communities to address any vaccine hesitancy. “In terms of organising mobile clinics, going to the community, putting up posters, building a relationship, the government should do this actively,” said Karpagam.