










On April 17, while inaugurating a charity hospital in Surat, Prime Minister Narendra Modi announced that the government intended to move a law to ensure that doctors prescribe medicines by their generic names only. The proposal has generated a heated conversation in the media and in the pharma industry.
Generics are medicines on which patents have expired. They are sold either as branded products or as unbranded products under their generic names. These generic names are internationally agreed short names called International Non-Proprietary Names. For example, paracetamol is the name for a pain relieving and fever reducing medication and Crocin is one brand name of paracetamol. For the purposes of this article, we will refer to unbranded generics simply as generic medicines.
The suggestion that doctors must write prescriptions in generic names is based on the idea that products sold as unbranded generic medicines are cheaper than others. This premise itself is not true for all generic medicines all the time. Retail pharmacists, in turn, have little incentive in stocking and selling low-price generic medicines since they have lower profit margins. Retail pharmacies have also no interest in selling low-priced branded medicines unless they are fast moving too.
In 2008, the government launched a chain of pharmacies called Jan Aushadhi to supply inexpensive generic medicines. In the last nine years, only a few such stores have been operational and they often have had stockouts and other problems. India has seven lakh retail pharmacy shops and still many rural areas are underserved. There are fewer than 10,000 Jan Aushadhis. A person seeking these medicines in a city would likely have to go to one of these few Jan Aushadhi stores negotiating dense traffic in an urban jungle or travel from a village to the nearby town – all to save a few rupees. This would only make sense for someone buying medicines for three to six months for a chronic condition like diabetes or hypertension.
Advocates of rational therapy and comprehensive public health originally preferred generic medicines to branded medicines because brands are more expensive. The price of a branded medicine includes the manufacturer’s marketing costs spent on “educating” the prescribing doctor. This “education” or drug promotion often extends to gifts and paid holidays and foreign jaunts for doctors. Companies also undertake brand promotion to distinguish their product from a rival’s – both being the same out-of-patent drug – or to distinguish it from a generic medicine with the claim of better quality than the chemically identical drug made by a small- or medium-scale pharmaceutical enterprise.
Generics, brands and quality
The size of a company does not necessarily ensure that the quality of its drugs is better or is as per regulatory norms. Quality is a function of how much a pharmaceutical company cares for the patient and for its reputation. Big products of well-known companies routinely get hauled up by state food and drug administrations for poor quality or for failing in some parameter listed in the pharmacopeia.
Drug quality can also be affected by factors outside the manufacturer’s control – the transport from the factory through the warehouse to the trade chain and onwards to storage facilities at the hospital or at the patient’s home.
The only way that a regulatory authority can systematically ensure good quality of medicines over a sustained period of time is strict quality control, audits and deterrent punishment of companies violating regulatory standards. Neither prescribing doctors nor patients can, normally, second guess the quality of branded or generic medicines without actual testing. .
What’s the price difference?
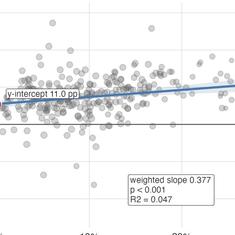
It is generally true that generic name products are less expensive than their brand equivalents. Big companies also make generic name products at very competitive prices. Generic medicines of quality compliant companies work as well as their big branded equivalents, and indeed they do and why not – for the process of manufacture is the same.
The total domestic pharmaceutical formulations market is about Rs one lakh crore. The market for generic name medicines is worth about Rs 10,000 crore or 10% of the domestic pharmaceutical formulations market. Medicines on the National List of Essential Medicines 2015 that are under price control constitute less than 12% of the total market of Rs one lakh crore. Another four percent of the market are useful medicines that have been put under price control by the government under Para 19 of the Drug Price Control Order 2013. .
At least 90% of the domestic Indian pharmaceutical market, therefore, consists of sale of branded products. If the government does institute a rule that doctors must prescribe only generic names, a patient will, in most cases, still end up buying a branded drug because as already pointed out generic medicines have low margins and therefore unlikely to be stocked by the retail pharmacist. This therefore does not ensure that the cost of his medication will come down by generic name prescriptions.
Doctors could end up writing an “official” prescription of only generic names and write an “unofficial” one recommending particular brands.
Also the pharmacist cannot legally substitute a generic for a brand, or brand for a generic, or brand for another brand. This law needs to be changed.
")
The market for fixed dose combinations is about 45% of the total market and worth about Rs 45,000 crores. To prescribe these medications under generic names, a doctor will have to write explicitly the generic constituents of the fixed dose combination in every prescription. For example, a doctor writing a prescription for Corex, will have to write chlorpheniramine maleate and codeine phosphate, or amoxicillin plus clavulanic acid instead of Augmentin. These are simpler medications. Many fixed-dose combinations like multivitamin products have between three and 10 ingredients. So for at least for 45 % of the market, the move to get prescribing doctors to write prescriptions in generic names will be a non-starter.
Duties of doctors
It is for some of these reasons that the September 2016 amendment to the Indian Medical Council’s Code of Conduct that advises generic prescription by doctors as part of their “duties and responsibilities”, has gone nowhere. If the intention of the amendment was serious, it should have stated upfront that it is mandatory for doctors to prescribe by generic names failing which they would be liable for prosecution. The amendment also does not state that doctors should prescribe only in generic names.
In the eight months since September 2016, no doctor has been hauled up for not prescribing in generic names and not complying with their prescribed duties and responsibilities. Presumably because nobody made a complaint to the Medical Council of India.
The other requirement of the September 2016 amendment that as part of their duties, doctors must “ensure that there is a rational prescription and use of drugs” also seems to be a non-starter again because a significant part of sales are irrational fixed dose combinations.
Once again, in announcing a radical sounding policy, the government has missed the devil in the details as well as the bigger picture. It is not really clear in the light of the above problems, how the government will ensure compliance without making other systemic changes we suggest below.
The big picture
The larger goal of such announcements like the one the PM made in Surat ought to be affordable access to quality medicines as part of free universal access to healthcare services. With the government’s push for privatisation and insurance-based access, the dream of universal health care for all seems to be receding.
To actually have better access to medicines, we need, at the minimum, the following:
- All formulations, representation and dosages of an enlarged list of essential and life-saving drugs to be put under price control.
- The market must be rid of all currently licensed irrational fixed dose combinations and useless and/or harmful medicines.
- The method of fixing price control in Drug Price Control Orders 2013 must be changed to a cost-based ceiling price determination. The current simple average formula legitimises high margins of up to 3000% over the cost of the product. So, methods of price control also need much more fine tuning.
- Laws for enabling substitution of generic and branded equivalents by pharmacists need to be introduced.
- A free medicine and diagnostics scheme in all states on the lines of such programmes in Tamil Nadu and Rajasthan.
- A fully functioning public health system with free healthcare for all like in the United Kingdom, Canada and Scandinavian countries.
- No brands for medicines that are out of patent as is the practice in well regulated countries.
- Briefer officially approved trade names for all rational fixed dose combinations so that doctors do not have to painfully write out the generic names of their multiple constituents.
- Creative use of government use compulsory licence provisions in the Patents Act to ensure competition in costly patented drugs and thereby make them less costly.
The writer works with LOCOST, Vadodara and the All-India Drug Action Network.