











India has overtaken Brazil and become the second-worst affected country in the world by the coronavirus pandemic, with more than 4 million cases. Covid-19 had mostly remained in India’s cities, but the disease is now spreading to rural India – an area with over 850 million people and far worse healthcare.
The reason for this shift appears to be migrant workers who have been returning to their villages since lockdown was eased at the end of June. The medical response to stop the spread and treat those infected has been inadequate, according to media reports.
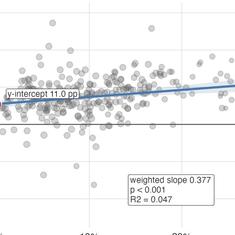
With one trained doctor for every 1,497 people, against the World Health Organization recommended one per 1,000, and public health expenditure for 2018 at just 1.3% of the gross domestic product, India faces an uphill struggle in dealing with the pandemic. While two-thirds of India’s population lives in rural areas, there are almost four times as many health workers per person in cities.
Most rural communities rely on untrained health workers. Over two-thirds of these rural health providers have no formal medical training but remain the only option of medical support for most of the rural population.
Covid stigma
This situation is worsened by the stigma and misinformation that surrounds Covid-19 in India. Fear of the virus has led to widespread mistrust of trained healthcare professionals. Indian doctors have reported being evicted from rented accommodation and others have been violently targeted in some slum communities. The misconception is that health professionals are sources of infection and that they will force people to be removed from their families into quarantine centres. These centres are viewed with suspicion and fear.

The stigmatisation of those infected or suspected to have Covid-19 is likely to result in unreported cases. And, indeed, some reports suggest that this is taking place. This means the situation can only get worse for Covid-19 victims and is undermining efforts to mitigate the pandemic.
In the long term, it threatens India’s recovery and progress, with the potential for many people to become debilitated with illness and economic hardship. In rural India, basic preventative measures of washing hands pose challenges because of the lack of access to clean running water.
Trust in and cooperation with the state, health professionals, or law enforcement agencies is key in the context of a pandemic. This is evidenced in countries such as Germany, South Korea and Taiwan, where trust is high, as well as the Indian state of Kerala and India’s biggest slum Dharavi in Mumbai, where citizens have cooperated and followed the guidelines. In each of these examples, the spread of the virus has been halted and controlled by a rigorous approach of test, track and trace.
In a parliamentary democracy, the bedrock of this approach is the willingness of the people to cooperate, accept responsibility and have confidence in the system. These three pillars, in turn, are anchored in the trust citizens have in the government machinery delivering public services. India’s pandemic response has made it clear how feeble such trust really is.
Trust in a pandemic
The situation in India has highlighted the weaknesses of public healthcare provision. India requires more resources to expand the pool of trained doctors accessible to its majority rural population and improve the trust people have in them.
Perhaps making careful use of informal health practitioners could be one way to do this. While the treatment they provide is often unsafe, most are usually trusted. My research into a women’s self-help network, conducted over eight years between 2009-17 in rural Bihar, India, suggests that many rural people have unreserved trust in their local village informal health practitioner. This is also echoed in other states of India.

These practitioners are not trained, and often patients end up being taken to the city at great expense. The villagers in my research were aware of these limitations but valued the support and immediate access, which can be lifesaving.
I witnessed an informal practitioner removing a bone from the throat of an elderly man using crude iron tongs. The man had been taken for dead by his family after severely choking as he ate.
I think that this faith in the informal practitioner could be harnessed, allowing the trust gap between people and the agencies delivering public health services to be bridged. With correct messaging, this could help overcome stigmatisation of Covid-19, compliance with public health measures and belief in medical professionals. My in-depth interviews with informal practitioners showed that many of them would like further professional training.
There is scattered evidence of informal practitioners leading Covid-19 preventative measures in some villages. A coordinated effort to train village practitioners, and creating a network of informed health workers that have community trust, could boost pandemic support in rural India.
Others have suggested this, but using trust as a key pillar to improve public health within scarce resources offers a novel approach. In the long run, this network of trained public health workers could improve healthcare in rural India.
Meera Tiwari is a Reader in International Development at the University of East London.
This article first appeared on The Conversation.