









When we think of the big health challenges, we may think of conquering cancer, heart disease, diarrhoea or pneumonia. These are certainly the big killers today. But we probably don’t think of mundane daily conditions such as backaches, neck pains or migraines. Pain does not kill people. Yet, every fifth person is likely to be suffering from some kind of pain, according to estimates of the World Health Organisation’s Global Burden of Disease study.
More than 20% of the world’s people have headaches, more than 13% have migraines, 7% have lower back pains, almost 5% have neck pains, and 3% have osteoarthritis, the study said.
Chronic pain is defined as any pain that lasts for more than three months. By some estimates, it affects at least 10% of the world’s population, although this might be an underestimation due to lack of representative and reliable global data.
India’s painful picture
In India, there is a serious dearth of data on pain. The only nationally representative study that provides some insights is the World Health Organisation’s Study of AGEing and Adult health or SAGE conducted in 2007 in six states – Assam, Karnataka, Maharashtra, Rajasthan, Uttar Pradesh and West Bengal. Through face-to-face interviews and self-reporting, the study collected evidence on various health conditions. One of these conditions was arthritis, a condition commonly known to cause pain and stiffness of joints.
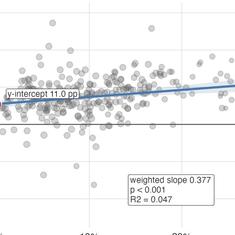
Seven per cent of the 4,665 respondents below the age of 50 reported that they had been diagnosed with arthritis. But when a set of questions about symptoms were posed, the prevalence was found to be higher, at 9%. Women had higher prevalence of arthritis than men and yet fewer women underwent treatment. Similarly, those from the lowest wealth quintile – the 20% of population that is the most economically backward as determined by their income, assets, household conditions and other factors – were more likely to have arthritis than those from the highest quintile but were less likely to get it treated.



Among the 6,557 adults aged over 50,the overall prevalence of arthritis was much higher than those below 50 – 18% self-reported and 23% based on symptoms. There was much more arthritis among older women than older men and but the women were less likely to get treated. Although there was not much difference in prevalence between older adults from the lowest and the highest wealth quintiles, poor people older than 50 received much less treatment than the richer adults in the same group. As we would expect, the many forms of inequality in India, of caste, gender, and class, affect and shape the experience and treatment of pain.


Chronic neglect
Despite its ubiquity, pain is grossly under-treated and greatly neglected by health systems across the world. One of the main reasons, many have argued, is its multifaceted, interdisciplinary and even ambiguous nature. There are so many things to consider when talking about pain – whether it is acute or chronic, whether is it regional or widespread in the body, and what its exact causes and pathways are. Often very little or nothing is known. This complexity and uncertainty perplex biomedicine, the dominant model of healthcare and health agendas across the world. Numerous studies have documented that experiences and expressions of pain that do not fall into neat predefined categories have been met with scepticism or even delegitimised.
This is particularly true for the intersection of pain and gender. The fact that women are at a greater risk of most common forms of pain than men are has been proven by several epidemiological, clinical and laboratory as well as sociological and anthropological studies. Yet, a large body of literature shows that even in the best functioning health settings where accessibility is not as big an issue as it is in India, women suffering from pain struggle to be taken seriously. Many illness narratives of women revolve around their difficult interactions with medical systems, concerns related to self-perceptions and fulfilling gender roles, and everyday negotiations of living with pain.
One of the reasons why medical systems are unable to deal with complexities of pain is that doctors are hardly trained for it. Judy Foreman in her book A Nation in Pain: Healing Our Biggest Health Problem reports that in 80% of the world, pain and pain management are not taught in medical schools at all. A 2011 study of 117 medical schools in the United States and Canada found that the median number of teaching hours allotted to pain was just nine for the US, while it was 18 for Canada.
No magic bullet
Social scientists who study pain, however, argue that the problem lies not only at execution, but also at the very way in which pain is conceived and understood. It is being increasingly acknowledged that health and illness are as much socially determined as biologically. This may be especially true for pain. Social processes related to gender, work, food and nutrition, caste and ownership of assets play an important role in the way pain is embodied and how it persists.
For instance, in one of the pioneering works in India, researchers showed how back pain is in fact a feminine affliction. Having to adopt “proper” monotonous postures as adolescents, bending for long hours for work in homes or in factories and having very low access and intake of calcium-rich foods, all this makes women’s bones fragile and upsets the architecture of the back balanced by vertebrae, muscles and ligaments, causing back pain.
In Pain: A Political History Keith Wailoo shows us that pain is a political issue too. Looking at the US political history and the divide between conservatives and liberals through the theme of pain, the book posits that whose pain is real and deserves relief is not just a clinical or scientific question but “a legal puzzle, a heated cultural concern, and an enduring partisan issue”. The history of pain, Wailoo argues, is about how the micro world of medicine and the macro sphere of politics intertwine to determine the kind of relief those in pain will get, making pain management a fraught political exercise.
A case in point is the inequitable global distribution of pain control and care. High-income countries with less than 15% of the world’s population account for more than 90% of the global consumption of morphine, an essential pain medication.The Access to Essential Medicines brief of the American Cancer Society reports that while low- and middle-income countries have 74% of deaths of people who remained untreated for pain while suffering from cancer and AIDS, they consume only 7% of medical opioids. India has 23% of these deaths of people who die from AIDS or cancer untreated for pain – the second largest such group after sub Saharan Africa.
Intra-country inequality in care is well known too. WHO SAGE 2007 showed that while Indian rural respondents in both below 50 and above 50 age groups had higher prevalence of arthritis, they were less likely to receive treatment than their urban counterparts.
But lack of access to essential medication is only the small part of a large and complex problem. Solutions to the most pressing health problems are often found outside the realm of medicine and healthcare services, something that the WHO’s Commission on Social Determinants of Health emphasised. Pain is one such problem, and it has to urgently become a global and national public health priority. This would mean shifting attention and resources to address the high incidence and prevalence of all forms of pain, and their links to gender, caste, poverty and work.
The writer is pursuing her MPhil at the Centre of Social Medicine and Community Health, Jawaharlal Nehru University.
This is the first part of a series on forms of pain that are not understood well or are ignored or dismissed as minor health issues. Read the series here.